Cologuard vs. Colonoscopy
Hi! This is my second research project with Undergraduate Research Society.
Assessing the Clinical Effectiveness of Cologuard vs. Colonoscopy in Early Detection of Colorectal Cancer.
🔬 Chandler Castillon, Lauren Song, Amanda Martin, Shriya Anand, Samia Khan, Riya Pandey, Praval Ghanta
Presented at: Undergraduate Research Conference at the University of South Florida.
Timeline: Aug 2024 - April 2025
Key Tools: Rayyan
Quick Links: View Poster
{kind=link}
Note: Use a desktop browser to view the interactive table of contents.
Research Overview
Abstract
In the past ten years, there has been a rise in the implementation of non-invasive colon cancer screening such as multitarget-stool DNA tests (MT-sDNA), also known as cologuard, fecal immunochemical tests (FIT), and tumor/blood based markers. This literature review aims to assess the clinical effectiveness of multi-target stool DNA tests (cologuard) versus the clinical effectiveness of a colonoscopy. Thirty-six articles were obtained using the reference management software, Endnote, and the National Institute of Health’s medical database to locate articles relating to cologuard/MT-sDNA and colonoscopies. This review found that cologuard was more effective at detecting precancerous and cancerous growths at a higher specificity but lower accuracy than colonoscopy. Additionally, adherence to preparation levels affected colonoscopy detection rates. Conducting a MT-sDNA test followed by a colonoscopy is far more effective at reducing colorectal cancer (CRC) incidence and mortality. The results obtained demonstrate that MT-sDNA tests are slightly more effective at detecting colon cancer and precancerous growths, however, without a follow-up colonoscopy, growths that were detected cannot be removed. By combining both MT-sDNA tests and colonoscopies together, CRC incidence and mortality can dramatically decrease.
Introduction
Colorectal cancer (CRC) is a serious public health concern and remains among the leading causes of cancer mortality globally. Screening for early detection of colorectal cancer is crucial in the prevention of incidence and mortality.
Two common employed CRC screening methods are colonoscopy and multi-target sstool DNA (MT-sDNA), or Cologuard. Both methods are to detect CRC at an early stage to improve patient outcomes. Colonoscopy is an invasive procedure in which a felxible tube with a camera is inserted into the colon to visually inspect the whole bowel for irregularities. It offers the ability to immediately remove detected polyps and is generally recommended every ten years for average-risk patients. In contrast, the Mt-sDNA test is a non-invasive stool test that detects occult blood and genetic markers for CRC. This testing is conducted at home and does not involve sedation or bowel prep and is typically recommended every three years.
Although Cologuard can identify aberrant blood and DNA linked to precancerous lesions and cancer with convenience, it may miss some advanced adenomas and has a greater false-positive rate. Colonoscopy enables direct vision, biopsy, and removal of polyps, offering advantages for both diagnosis and prevention due to higher sensitivity.
The purpose of this research project is to help determine the clinical effectiveness of Cologuard and colonoscopy when screening for colon cancer.
Methods and Materials
PRISMA 2020 flow diagram for new systematic reviews which included searches of databases and registers only
Figure 1 - Flowchart of screening proceses
Exclusion and Inclusion Criteria
- Exclusion: Case studies, testing procedures irrelevant to colonoscopy, surveys, data prior to 2000, literary reviews, animal studies.
- Inclusion: Treatment effectiveness, broad population, limiting factors, colonoscopy primary sources, details’ statistics about colorectal cancer, Cologuard, multitarget stool DNA testing, stool-based DNA methylation test.
Results
Hover for details.
Figure 2
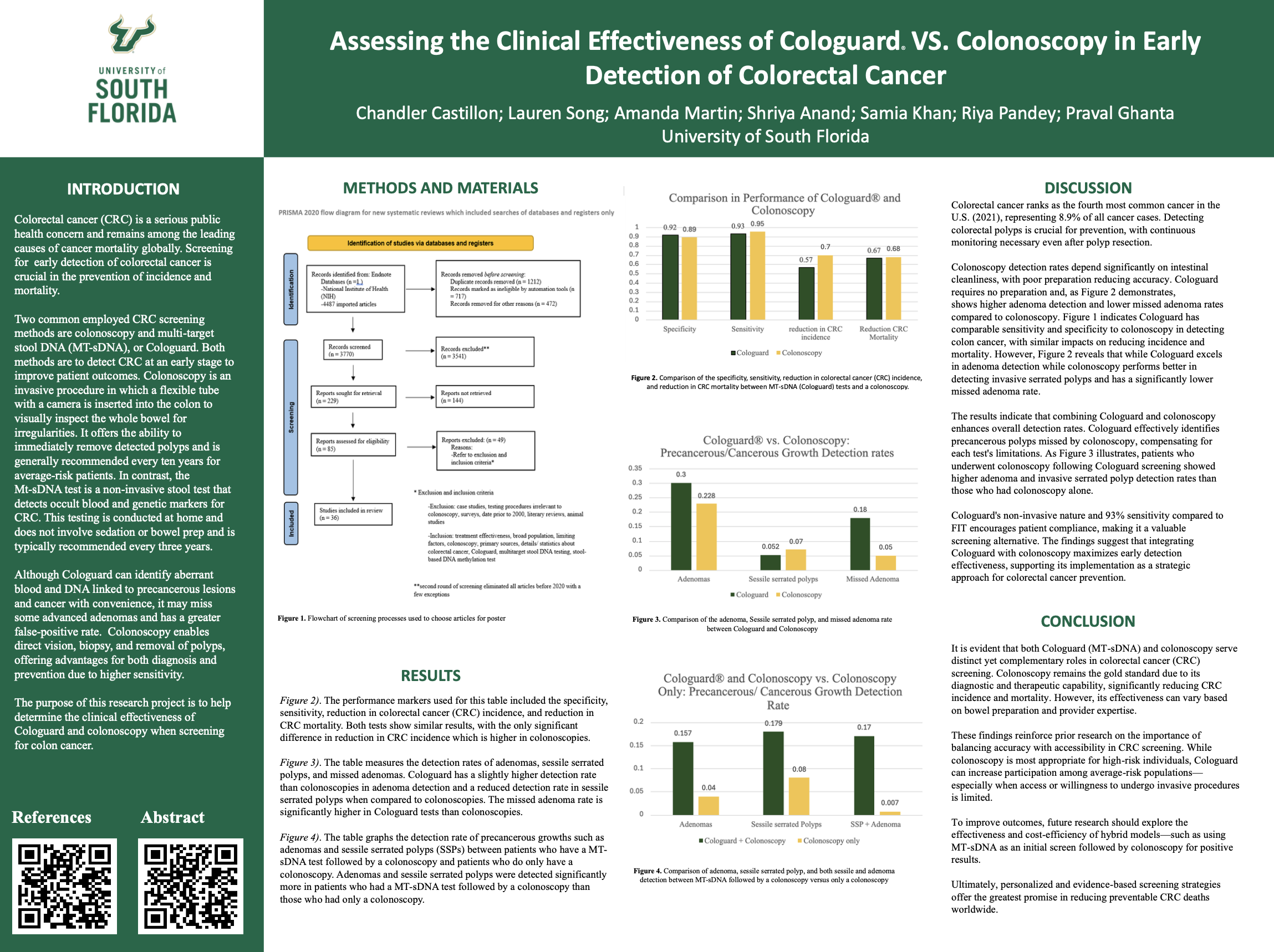
Comparison of the specificity, sensitivity, reduction in colorectal cancer (CRC) incidence, and reduction in CRC mortality between MT-sDNA (Cologuard) tests and a colonoscopy.
Figure 2 The performance markers used for this table included the specificity, sensitivity, reduction in colorectal cancer (CRC) incidence, and reduction in CRC mortality. Both tests show similar results, with the only significant difference im reduction in CRC incidence which is higher in colonoscopies.
Figure 3
Comparison of the adenoma, sessile serrated polyp, and missed adenoma rate between Cologuard and Colonoscopy.
Figure 3. The table measures the detection rates of adenomas, sessile serrated polyps, and missed adenomas. Cologuard has a slightly higher detection rate than colonoscopies in adenoma detection and a reduced detection rate in sessile serrated polyps when compared to colonoscopies. The missed adenoma rate is significantly higher in Cologuard tests than colonoscopies.
Figure 4
Comparison of adenoma, sessile serrated polyp, and both sessile and adenoma detection between MT-sDNA followed by a colonoscopy versus only a colonoscopy
Figure 4. The table graphs the detection rate of precancerous growths such as adenomas and sessile serrated polyps (SSPs) between patients who have a MT-sDNA test followed by a colonoscopy and patients who do only have a colonoscopy. Adenomas and sessile serrated polyps were detected significantly more in patients who had a MT-sDNA test followed by a colonoscopy than those who had only a colonoscopy.
Discussion
Colorectal cancer ranks as the fourth most common cancer in the U.S. (2021), representing 8.9% of all cancer cases. Detecting colorectal polyps is crucial for prevention, with continous monitoring necessary even after polyp resection.
Colonoscopy detection rates depend significantly on intestinal cleanliness, with poor preparation reducing accuracy. Cologuard requires no preparation and, as Figure 2 demonstrates, shows higher adenoma detection and lower missed adenoma rates compared to colonoscopy. Figure 1 indicates Cologuard has comparable sensitivity and specificity to colonoscopy in detecting colon cancer, with similar impacts on reducing incidence and mortality. However, Figure 2 reveals that while Cologuard excels in adenoma detection while colonoscopy performs better in detecting invasive serrated polyps and has a significantly lower missed adenoma rate.
The results indicate that combining Cologuard and colonoscopy enhances overall detection rates. Cologuard effectively identifies precancerous polyps missed by colonoscopy, compensating for each test’s limitations. As Figure 3 illustrates, patients who underwent colonoscopy following Cologuard screening showed higer adenoma and invasive serrated polyp detection rates than those who had colonoscopy alone.
Cologuard’s non-invasive nature and 93% sensitivity compared to FIT encourages patient compliance, making it a valuable screening alternative. The findings suggest that integrating Cologuard with colonoscopy maximizes early detection effectiveness, supporting its implementation as a strategic apporach for colorectal cancer prevention.
Conclusions
It is evident that both Cologuard(MT-sDNA) and colonoscopy serve distinct yet complementary roles in colorectal cancer(CRC) screening. Colonoscopy remains the gold standard due to its diagonostic and therapeutic capability, significantly reducing CRC incidence and mortality. However, its effectiveness can vary based on bowel preparation and provider expertise.
These findings reinforce prior research on the importance of balancing accuracy with accessibility in CRC screening. While colonoscopy is most appropriate for high-risk individuals, Cologuard can increase participation among average-risk populations-especially when access or willingness to undergo invasive procedures is limited.
To improve outcomes, future research should explore the effectiveness and cost-efficiency of hybrid models-such as using MI-sDNA as an initial screen followed by colonoscopy for positive results.
Ultimately, personalized and evidence-based screening strategies offer the greatest promise in reducing preventable CRC deaths worldwide.